
The lecture below can be accessed on the Disease Management section of the Cleveland Clinic, under Allergy and Immunology (to go to this link and see others in the series, please click here)
Occupational Asthma
Mark Aronica
Published: May 2014
Definition
The definition of occupational asthma (OA), much like the definition of asthma itself, has changed over the years; therefore, it is difficult to determine the prevalence of the disorder (see below). The current consensus definition is as follows: “Occupational asthma” is a disease characterized by variable airflow limitation and/or airway hyperresponsiveness due to causes and conditions attributable to a particular occupational environment and not to stimuli encountered outside the workplace. Two types of OA are distinguished by whether or not they appear after a latency period: (1) immunologic, characterized by a latency period, encompassing (a) that caused by high- (HMW) and low-molecular-weight (LMW) agents for which an immunologic (IgE) mechanism has been proven, and (b) that caused by agents (e.g., western red cedar) for which a specific immune mechanism has not been identified. (2) Nonimmunologic, i.e., irritant-induced asthma (IrIA) or reactive airways dysfunction syndrome (RADS), which may occur after single or multiple exposures to nonspecific irritants at high concentrations.1 A second, related form of OA has been termed “work-aggravated asthma.” In this instance, preexisting asthma is aggravated by a workplace exposure. Although work-aggravated asthma is not specifically addressed in this chapter, it is worth noting that the evaluation of all cases of asthma should include a detailed environmental history regarding exposures in both the home and the workplace.
Prevalence
Occupational asthma is a part of a larger category of diseases known as occupational respiratory diseases and includes occupation-induced rhinitis and laryngitis, tracheitis, bronchitis and bronchiolitis, chronic obstructive pulmonary disease, lung cancer, and interstitial diseases such as fibrosis and granuloma formation.2 Although both physicians and the lay public are aware of other occupational lung disorders such as silicosis and asbestosis (see Disease Management chapter on Occupational Lung Disease), OA is the most prevalent occupational lung disease in industrialized countries. Findings regarding the significance of occupation as a cause of asthma vary based on the definition used and the methods for patient selection. In addition, people who develop OA often leave the industry in which the illness began (a bias known as the “healthy worker effect”), even when OA has not yet been diagnosed. In general, asthma affects 5% to 10% of people worldwide, and it is estimated that 2% to 15% of asthma may be occupational in origin.
The incidence of OA also varies with specific exposures. OA has been reported in 8% to 12% of laboratory animal workers, 7% to 9% of bakers, and 1.4% of healthcare workers exposed to natural rubber latex. Even these percentages vary significantly depending on the study cited. Farmers, painters, plastic and rubber workers, and cleaners (caretakers, window cleaners, chimney and road sweepers) are at greatest risk for developing asthma.3 Over the past several years there has been an increased awareness, and growing evidence that cleaners are at increased risk of developing OA and other respiratory disorders.4 The use of spray products seemed to impart a higher risk than other types of cleaners. While there was a good deal of variabiltiy as to the identified cause, the most common cleaners linked to OA were chlorine bleach, ammonia, and air freshening sprays.
Pathophysiology
Like childhood asthma, OA is the result of interactions between multiple environmental and genetic factors. Some of the known environmental factors include the route, duration, and intensity of exposure, and the substance (or agent) to which the subject is exposed. Using the definition given above, OA can be divided into immunologic causes (associated with a latency period) and nonimmunologic causes. Agents associated with an immunologic cause can be further divided into HMW agents, usually allergens such as proteins from laboratory animals, flour, or plants, or LMW agents, usually chemicals such as isocyanates, biocides, or drugs.
Occupational Asthma with a Latency Period
HMW agents can induce an immunoglobulin E (IgE) response in susceptible individuals and can cause asthma by an IgE-mediated mechanism, similar to that seen in a patient with atopic asthma. The bridging of IgE molecules by antigen leads to mast-cell degranulation and the initiation of an inflammatory cascade that results in airway inflammation and airway hyperresponsiveness. It is therefore not surprising that patients with atopic asthma or patients with a family history of atopy are at increased risk for developing OA from exposure to HMW agents. Smoking is also a risk factor for sensitization.
The pathogenic mechanisms of LMW agents are less well understood; however, there appear to be several mechanisms, both immunologic and nonimmunologic, that can lead to OA. LMW agents probably act as haptens, combining with human proteins in the respiratory tract to become complete immunogens. Atopy and smoking are not risk factors for OA caused by LMW agents as they are for OA caused by HMW agents. Some of the better-studied agents include isocyanates and plicatic acid. Isocyanates are found in paints and are involved in the manufacture of plastics, rubber, and foam, whereas plicatic acid is the causative agent in asthma caused by western red cedar. Specific IgE for isocyanates or plicatic acid is found in only a small percentage of patients with documented disease. However, the detection of specific IgE may be a marker of exposure and not of disease.5
Activated T cells also play an important role in the pathogenesis and in the inflammation of OA as they do in other forms of asthma. Bronchial biopsies of patients with isocyanate- or red cedar-induced OA show many activated T cells.6,7 In addition, several recent studies have shown associations between HLA class II antigens and various types of OA.8
Other mechanisms by which LMW agents cause OA include direct pharmacologic actions of these agents. Isocyanates can block beta 2-adrenergic receptors, and high concentrations of plicatic acid can activate complement. Moreover, isocyanates and other agents can stimulate sensory nerves, leading to the release of substance P and other neuropeptides. They can also inhibit the neutral endopeptidases that normally inactivate these substances. This affects a variety of cells in the airways, resulting in cough, smooth muscle contraction, and mucus production.
Table 1 shows some of the more common causes of OA associated with a latency period.
Table 1: Common Agents that Cause Occupational Asthma with Latency
| High-Molecular-Weight Agents |
|---|
| Cereals |
| Animal-derived allergens |
| Enzymes |
| Gums |
| Latex |
| Seafoods |
| Low-Molecular-Weight Agents |
| Isocyanates |
| Wood dusts |
| Anhydrides |
| Amines |
| Fluxes |
| Chloramine-T |
| Dyes |
| Persulfate |
| Formaldehyde, glutaraldehyde |
| Acrylate |
| Drugs |
| Metals |
Occupational Asthma Without Latency
The mechanisms of IrIA or RADS are also poorly understood. IrIA is a nonimmunologically induced asthma that occurs without a latency period. It typically occurs after a brief, high-intensity inhalation exposure followed by the acute onset of persistent respiratory symptoms and ongoing airway hyperresponsiveness. It is postulated that extensive denudation of the airway epithelium occurs, resulting in airway inflammation due to the loss of epithelium-derived relaxing factors, exposure of nerve endings leading to neurogenic inflammation, and nonspecific activation of mast cells with release of inflammatory mediators and cytokines.9 Ammonia, chlorine, and sulfur dioxide are the most frequent causes of IrIA, although the list is extensive.
Signs and Symptoms
The signs and symptoms of OA may be identical to those of other forms of asthma. In patients whose OA is caused by HMW agents, rhinitis or rhinoconjunctivitis often precedes the onset of asthma symptoms by 1 year or more. In contrast, IrIA or RADS has a characteristically distinct presentation. The exposure is typically acute, singular, and extreme, often involving some type of accident or chemical spill. There is no latency period, and symptoms of airway obstruction are immediate or develop within a few hours of exposure.
In patients with OA with a latency period, symptom improvement has been noted over a weekend with 24 to 48 hours of work absence in about 70% of patients and up to 90% of workers with vacation leaves of 7 to 10 days.10 Symptom patterns can also be very similar to those seen in non-OA and include early, late, and dual responses. Early responses are seen within minutes of exposure, reach maximal severity within 30 minutes, and resolve within 1 to 2 hours. Late responses may occur after 4 to 6 hours, peak around 8 hours, and resolve after 24 hours. Dual responses involve both early response with complete or near-complete recovery followed by a late phase.
Diagnosis
The diagnosis of OA should be considered in all working-age individuals with new-onset asthma or worsening asthma. A detailed history of occupational and potential occupational exposures is just as important as identifying environmental triggers when evaluating an asthmatic patient. Although many patients will themselves relate their symptoms to the workplace, many other cases of OA are recognized only because the physician performed a detailed environmental history. Common screening questions include the following: What are your workplace exposures? When during the work shift or workweek do symptoms develop? Do symptoms improve during the weekend and over vacations? Do other workers have similar symptoms? The history can be supplemented with material safety data sheets from the workplace and can be compared with agents known to cause OA. A worksite visit by the physician or by an occupational hygienist might also provide helpful information.
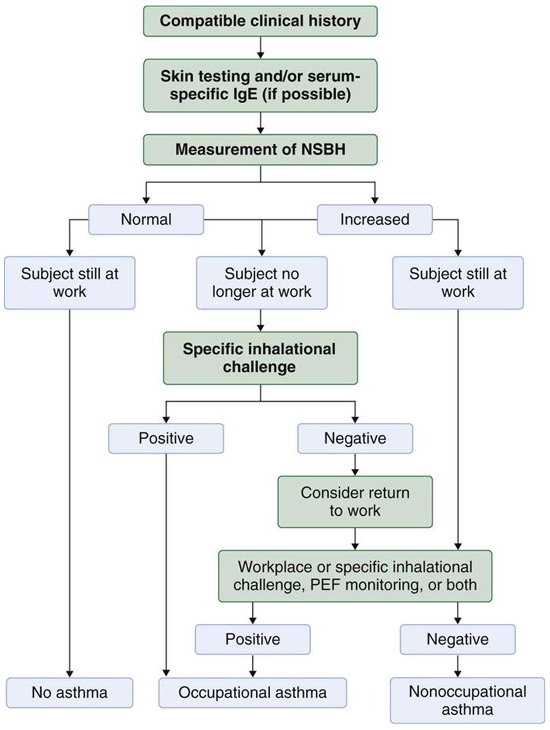
Although taking a good occupational history is important in establishing a link between symptoms and potential workplace exposures, a history by itself is inadequate to make the diagnosis of OA. Algorithms and information on the diagnosis of OA can be found below and in Figure 1.More detailed information may also be found in the references.11-13 If possible, skin testing and/or specific IgE assessment should be performed. This is generally most useful for the diagnosis of OA caused by HMW agents.
A determination of nonspecific bronchial hyperresponsiveness (NSBH) with methacholine or histamine challenge should be performed in all patients suspected of having OA. A negative challenge does not exclude OA if the patient has left the workplace some time ago and is now free of symptoms. However, a negative challenge performed when the patient is working and symptomatic can reasonably exclude the diagnosis of OA. Serial measurements of NSBH can also be useful. NSBH is typically worse after a period of exposure and can lessen after cessation of exposure. A minimum of 10 to 14 days after removal from the workplace exposure is recommended before retesting. A minimum threefold improvement in PC20 (dose of methacholine or histamine needed to cause a 20% decrease in the Forced Expiratory Volume in 1 second [FEV1]) while the patient is off work is significant; however, a lack of improvement in PC20 does not exclude OA.
Serial peak expiratory flow (PEF) self-monitoring with the subject at work and away from work for the same period is useful in obtaining objective information for the confirmation of OA. Current recommendations are for four daily measurements; the subject should perform three forced-expiratory maneuvers, and at least two should be within 20L/min of each other. All three readings should be recorded, but the best should be used for analysis. If a patient is taking inhaled corticosteroids, the dose should not be changed during the PEF monitoring period. All readings should be done prior to use of bronchodilators. Readings should be performed for 2 weeks at work during exposure to the suspected agent, and for 2 weeks away from the suspected agent.14,15 Having a motivated and compliant patient is essential for PEF monitoring to be useful.
The gold standard for the diagnosis and confirmation of OA is a specific inhalational challenge with the suspected agent. However, this requires specialized facilities and is available at only a few centers. In general, specific challenge tests are useful in the following circumstances: (1) when the diagnosis of OA remains in doubt after serial monitoring of PEF or NSBH; (2) when a patient clearly has OA but it is necessary to confirm the causative agent for correct management; and (3) when a new agent is suspected of causing OA.
Therapy
The most important aspect in the treatment of OA is environmental control. Continued exposure can lead to persistent and irreversible airway obstruction, whereas early removal offers the best chance at complete recovery. Other than environmental control, the management of OA is no different than that for non-OA. However, pharmacologic treatment is not effective in preventing deterioration of lung function in sensitizer-induced OA when subjects remain exposed to the causal agent. (For additional information on the management of asthma, see the Disease Management chapter, Asthma.)
In contrast, patients with RADS or IrIA without concurrent sensitization can usually return to the workplace if they have adequate pharmacologic control of their asthma and if there are appropriate occupational hygiene controls in place to prevent the likelihood of a repeat high-level respiratory irritant exposure.
Outcomes
The outcome in OA depends on many of the same elements that are involved with initial sensitization and include the nature of the agent, the concentration of exposure, the duration of exposure, and the smoking history as well as host-dependent factors. Factors predicting a worse outcome are lower PC20 at baseline, longer duration of exposure, and the interval since removal of the patient from exposure. As mentioned above, early removal offers the best chance at recovery. However, most patients with OA with latency do not recover, even after several years away from exposure. In addition, subjects with OA to HMW agents seem to have a less favorable outcome. The typical plateau for improvement in spirometry is around 1 year, whereas the plateau for improvement in NSBH occurs around 2 years.
The socioeconomic outcomes of OA also vary significantly. For example, a patient in Quebec diagnosed with OA is provided with full salary for up to 2 years, which is the estimated time required for retraining for a new occupation. A survey of 134 workers with OA examined 2 years after diagnosis found that 41 (31%) had found jobs with the same employer in which they were no longer exposed to the causal agent, and only 11 (8%) of workers were still unemployed.16 In contrast, a survey of 55 subjects in the United States with OA who were assessed an average of 31 months after removal from exposure found that 69% were still unemployed.17
Once the diagnosis of OA is made, that worker is 100% impaired for the job that caused the problem or for jobs with exposure to the same causative agent. It is recommended that long-term assessment of impairment should be performed 2 years after removal from exposure, when improvement tends to plateau. Guidelines for the assessment of permanent impairment due to asthma have been proposed by the American Thoracic Society.18
Summary
In summary, OA should be considered in any new or worsening case of asthma in working-age individuals. Although there are still many controversies regarding the diagnosis, pathophysiology, prognosis, and appropriate compensation for patients with OA, prompt recognition, diagnosis, and removal from the work environment are necessary to ensure the best possible outcome. Additional information on OA can also be found at www.osha.gov/SLTC/occupationalasthma/.
References
- Bernstein IL, Bernstein DI, Chan-Yeung M, Malo J-L. Definition and classification of asthma. In: Bernstein IL, Chan-Yeung M, Malo J-L, Bernstein DI, eds. Asthma in the Workplace. 2nd ed. New York, NY: Marcel Dekker; 1999:1–3.
- Beckett WS. Occupational respiratory diseases. N Engl J Med 2000; 342:406–413.
- Kogevinas M, Antó JM, Sunyer J, Tobias A, Kromhout H, Burney P; the European Community Respiratory Health Survey Study Group. Occupational asthma in Europe and other industrialised areas: a population-based study. Lancet 1999; 353:1750–1754.
- Zock J-P, Vizcaya D, Le Moual N. Update on asthma and cleaners. Curr Opin Allergy Clin Immunol 2010; 10:114–120.
- Frew A, Chan H, Dryden P, Salari H, Lam S, Chan-Yeung M. Immunologic studies of the mechanisms of occupational asthma caused by western red cedar. J Allergy Clin Immunol 1993; 92:466–478.
- Bentley AM, Maestrelli P, Saetta M, et al. Activated T-lymphocytes and eosinophils in the bronchial mucosa in isocyanate-induced asthma. J Allergy Clin Immunol1992; 89:821–829.
- Frew AJ, Chan H, Lam S, Chan-Yeung M. Bronchial inflammation in occupational asthma due to western red cedar. Am J Respir Crit Care Med 1995; 151:340–344.
- Taylor AJ. HLA phenotype and exposure in development of occupational asthma. Ann Allergy Asthma Immunol 2003; 90(5 suppl 2):24–27.
- Gautrin D, Bernstein IL, Brooks S. Reactive airways dysfunction syndrome, or irritant-induced asthma. In: Bernstein IL, Chan-Yeung M, Malo J-L, Bernstein DI, eds. Asthma in the Workplace. 2nd ed. New York, NY: Marcel Dekker; 1999:565–593.
- Tarlo SM, Boulet LP, Cartier A, et al. Canadian Thoracic Society guidelines for occupational asthma. Can Respir J 1998; 5:289–300.
- Malo J-L, Chan-Yeung M. Occupational asthma. J Allergy Clin Immunol 2001; 108:317–328.
- Chan-Yeung M, Malo J-L. Occupational asthma. N Engl J Med 1995; 333:107–112.
- Chan-Yeung M, Malo J-L, Tarlo SM, et al; American Thoracic Society. Proceedings of the first Jack Pepys Occupational Asthma Symposium. Am J Respir Crit Care Med 2003; 167:450–471.
- Burge PS MG. Physiologic assessment: serial measurements of lung function. In: Bernstein IL, Chan-Yeung M, Malo J-L, Bernstein DI, eds. Asthma in the Workplace. 2nd ed. New York, NY: Marcel Dekker; 1999:193–210.
- Moscato G, Godnic-Cvar J, Maestrelli P; for the Subcommittee on Occupational Allergy of European Academy of Allergy and Clinical Immunology. Statement on self-monitoring of peak expiratory flows in the investigation of occupational asthma. J Allergy Clin Immunol 1995; 96:295–301.
- Dewitte JD, Chan-Yeung M, Malo J-L. Medicolegal and compensation aspects of occupational asthma. Eur Respir J 1994; 7:969–980.
- Gassert TH, Hu H, Kelsey KT, Christiani DC. Long-term health and employment outcomes of occupational asthma and their determinants. J Occup Environ Med1998; 40:481–491.
- American Thoracic Society. Guidlines for the evaluation of impairment/disability in patients with asthma. Am Rev Respir Dis 1993; 147:1056–1061.